
 Hirsutism is a source of significant anxiety in women. While polycystic ovary syndrome (PCOS) or other endocrine conditions are responsible for excess androgen in many patients, other patients have normal menses and normal androgen levels (“idiopathic” hirsutism).
Hirsutism is a source of significant anxiety in women. While polycystic ovary syndrome (PCOS) or other endocrine conditions are responsible for excess androgen in many patients, other patients have normal menses and normal androgen levels (“idiopathic” hirsutism).The finding of polycystic ovaries on ultrasound is not required for the diagnosis of polycystic ovary syndrome (PCOS). Gonadotropin-dependent ovarian hyperandrogenism is believed to cause PCOS. However, mild adrenocorticotropic-dependent adrenal hyperandrogenism also is a feature in many cases.
Even women with mild hirsutism can have elevated androgen levels, and thus, they may benefit from a laboratory evaluation.
Laser treatment does not result in complete, permanent hair reduction, but it is more effective than other methods such as shaving, waxing, and electrolysis. It produces hair reduction for up to 6 months. The effect is enhanced with multiple treatments. Interestingly, a portable laser hair removal device is currently available from Amazon (this post is not a recommendation or endorsement of the product).
References:
Update on the management of hirsutism. Cleveland Clinic Journal of Medicine June 2010 vol. 77 6 388-398.
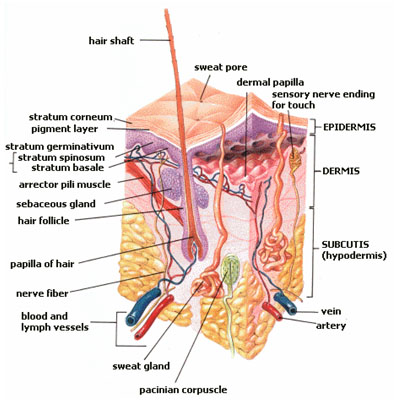
Image source: Skin layers. Wikipedia, public domain.
A home hair removal laser device is available without prescription from Amazon.com (not a recommendation to buy any product, see the link below). A similar device is available from Costco.




{kind=link}
{kind=link}
{kind=link}